Category: Males
-
NHS gender clinics do not meet quality assurance standards.
An operational and delivery review1 of adult gender clinics in England found that clinics lacked patient outcome data, had limited data reporting of inconsistent quality, and had minimal clinical audit. These failings put the clinics outside standard NHS quality assurance expectations.
These clinics also showed no signs of responding to the changing demographics of their referrals. Clinics made little effort to respond to the needs of this changing cohort, which was younger and more female than had previously been the case.
Some clinics reportedly carried out little or no knowledge-sharing or quality improvement work. Senior clinical leadership also steered some clinicians away from appropriate clinical curiosity, limiting opportunities to improve patient outcomes. In addition, many clinics were not well overseen by their local trust boards, nor by NHS England.
- Levy D, Operational and delivery review of NHS adult gender dysphoria clinics in England. https://www.england.nhs.uk/publication/operational-and-delivery-review-of-nhs-adult-gender-dysphoria-clinics-in-england/ ↩︎
-
All-cause mortality is higher for males taking estrogen than for men in general.
A retrospective cohort study1 of patients at an Amsterdam gender clinic found that all-cause mortality increased within a few years of beginning estrogen treatment and continued to increase over time. Men taking estrogen had an overall Standard Mortality Ratio (SMR) of 1.8 compared to men in general. The major causes of death included cardiovascular disease (21%), cancer (32%), infection-related disease (5%), and suicide (7.5%).
- de Blok CJ, Wiepjes CM, van Velzen DM, Staphorsius AS, Nota NM, Gooren LJ, Kreukels BP, den Heijer M. Mortality trends over five decades in adult transgender people receiving hormone treatment: a report from the Amsterdam cohort of gender dysphoria. Lancet Diabetes and Endocrinology. 2021 Oct;9(10):663-670. doi: 10.1016/S2213-8587(21)00185-6. Epub 2021 Sep 2. PMID: 34481559. ↩︎
-
Around one in six young people treated with cross sex hormones ceased treatment.
An exploratory study1 of adolescents and young adults in Canada and the US found that 16.8% of those receiving “gender affirming medical treatment” (puberty blockers and cross sex hormones) stopped “treatment” within around five years of declaring a “trans” or “non binary” identity.
Of those who discontinued treatment, 37.3% did so for health reasons. 32% ended treatment due to a change in gender identity. 12% were persuaded by health professionals or a partner to explore different ways of approaching their gender dysphoria.
Stopping treatment was associated with having a “non binary” identity. Both continuing and non-continuing cohorts had a mean age of 16.1 when “coming out”, but those discontinuing treatment were slightly older (22.1 vs. 20.9.)
- MacKinnon KR, Jeyabalan T, Strang JF, Delgado-Ron JA, Lam JSH, Gould WA, Cooper A, Salway T. Discontinuation of Gender-Affirming Medical Treatments: Prevalence and Associated Features in a Nonprobabilistic Sample of Transgender and Gender-Diverse Adolescents and Young Adults in Canada and the United States. Journal of Adolescent Health. 2024 Oct;75(4):569-577. doi: 10.1016/j.jadohealth.2024.05.015. Epub 2024 Jun 28. PMID: 38944803. ↩︎
-
Bone mineral density that declines during puberty blockade may not fully recover with cross-sex hormone treatment.
A cohort study1 of trans-identified people who had received puberty blockers and long-term cross sex hormones found that bone mineral density z-scores (which compare the patient with age- and sex-typical values) fell during puberty blockade, and did not fully recover following over a decade of cross-sex hormone treatment. This was especially the case for the lumbar spine of males receiving estrogen.
It is also notable that, of the original 143 eligible participants, only 75 completed this research. Of those who left the cohort, 6 (4%) had discontinued cross-sex hormone treatment and 27 (19%) could not be reached. These figures are consistent with high loss to follow up in other studies of so-called “gender-affirming care.”

- van der Loos MATC, Vlot MC, Klink DT, Hannema SE, den Heijer M, Wiepjes CM. Bone Mineral Density in Transgender Adolescents Treated With Puberty Suppression and Subsequent Gender-Affirming Hormones. JAMA Pediatrics. 2023 Dec 1;177(12):1332-1341. doi: 10.1001/jamapediatrics.2023.4588. PMID: 37902760; PMCID: PMC10616766. ↩︎
-
Boys receiving puberty blockers for gender dysphoria experienced irreversible changes to their testes.
A histological analysis1 of testicular tissue taken from boys receiving puberty blockers for gender dysphoria showed that the tissue showed abnormal development that was likely to be irreversible.

Samples were gathered as part of “fertility preservation surgery,” in which testicular tissue is harvested and preserved in hope that it will be able to produce sperm later. Every boy with gender dysphoria in the study had elected for this surgery due to inability or reluctance to ejaculate. This suggests the possible presence of various psychological and physical conditions that are unexplored in the research.
- Murugesh V, Ritting M, Salem S, Aalam SMM, Garcia J, Chattha AJ, Zhao Y, Knapp DJ, Kalthur G, Granberg CF, Kannan N. Puberty Blocker and Aging Impact on Testicular Cell States and Function. bioRxiv [Preprint]. 2024 Mar 27:2024.03.23.586441. Doi: 10.1101/2024.03.23.586441. PMID: 38585884; PMCID: PMC10996503. ↩︎
-
Depression symptoms got worse in children taking puberty blockers.
In a study1 of 94 children with gender dysphoria, aged 8-16 and beginning to take puberty blockers, depression symptoms were more likely to get worse than to improve over two years of treatment. Scores on the Beck Depression Inventory (BDI-Y) went from 72% average, 10% mildly elevated, 10% moderately elevated, and 8% severely elevated at baseline to 75% average, 7% mildly elevated, 14% moderately elevated, and 9% severely elevated after 24 months.
This study was conducted from 2016 to 2021 by Dr. Johanna Olson-Kennedy. In 2024, the New York Times reported2 Dr. Olson-Kennedy saying that publication of this research had been delayed because she feared that research showing that puberty blockers did not improve patients’ mental health would be “weaponized” against the use of puberty blockers by opponents of the practice. The report appeared as a pre-print, not peer-reviewed, in May 2025.
- Johanna Olson-Kennedy, Liyuan Wang, Carolyn F. Wong, Diane Chen, Diane Ehrensaft, Marco A. Hidalgo, Amy C. Tishelman, Yee-Ming Chan, Robert Garofalo, Asa E. Radix, Stephen M. Rosenthal, Emotional Health of Transgender Youth 24 Months After Initiating Gender-Affirming Hormone Therapy, Journal of Adolescent Health, Volume 77, Issue 1, 2025, Pages 41-50, ISSN 1054-139X, https://doi.org/10.1016/j.jadohealth.2024.11.014. ↩︎
- https://www.nytimes.com/2024/10/23/science/puberty-blockers-olson-kennedy.html
↩︎
-
IQ fell in a male patient whose puberty was blocked due to gender distress.
A case study1 of a male patient whose puberty was blocked at age 11 showed a decline in several measurements of intelligence over the following three years, including decline of 10 points in global IQ and 15 points in verbal comprehension.
Verbal comprehension showed a continuous decline. Other measurements showed some improvement after an initial decline, but never recovered to baseline levels. Processing speed index scores initially improved, but then fell below baseline.

- Schneider MA, Spritzer PM, Soll BMB, Fontanari AMV, Carneiro M, Tovar-Moll F, Costa AB, da Silva DC, Schwarz K, Anes M, Tramontina S, Lobato MIR. Brain Maturation, Cognition and Voice Pattern in a Gender Dysphoria Case under Pubertal Suppression. Frontiers in Human Neuroscience. 2017 Nov 14;11:528. doi: 10.3389/fnhum.2017.00528. PMID: 29184488; PMCID: PMC5694455. ↩︎
-
Men taking exogenous estrogen may be at higher risk of branch retinal vein occlusion.
In a case study1 of a man taking “gender-affirming” estrogen, a plausible causal link was suggested between exogenous estrogen and branch retinal vein occlusion (BRVO), based chiefly on existing established links between estrogen and cardiovascular risk. The study also suggests that trans-identified patients may be unwilling to stop using estrogen even when experiencing BRVO.
- Andzembe V, Miere A, Zambrowski O, Glacet-Bernard A, Souied EH. Branch retinal vein occlusion secondary to hormone replacement therapy in a transgender woman. J Fr Ophtalmol. 2023 Feb;46(2):148-151. doi: 10.1016/j.jfo.2022.07.024. Epub 2023 Jan 4. PMID: 36609071. ↩︎
-
Males taking estrogen may be at risk of keratoconus.
A case study1 of a 28 year old man taking “gender-affirming” estrogen suggested that such treatment may accelerate the progression of keratoconus.
- Carli M. Deitel, Kevin H. Chen, Ian C. Uber, Possible association of keratoconus progression with gender-affirming hormone therapy: A case report, American Journal of Ophthalmology Case Reports, Volume 30, 2023, 101850, ISSN 2451-9936, https://doi.org/10.1016/j.ajoc.2023.101850. ↩︎
-
Rates of gender-affirming surgeries in the US tripled from 2016-2019.
A cohort study1 of data from the Nationwide Ambulatory Surgery Sample and the National Inpatient Sample showed that 48019 patients in the US received some kind of “gender-affirming” surgery between 2016 and 2020. Numbers peaked at 13011 in 2019 then fell slightly to 12818 in 2020. The study’s authors attribute this decline to the impact of the COVID-19 pandemic though, meaning the historical peak may not have been reached by then. 7.7% of all patients (3678 of the total) were aged 12-18 at the time of their surgery. 405 of these surgeries on minors (2.4% of the whole study) were genital surgeries. More than half (52.3%, or 25099 patients) were aged 19-30.
- Wright JD, Chen L, Suzuki Y, Matsuo K, Hershman DL. National Estimates of Gender-Affirming Surgery in the US. JAMA Network Open. 2023;6(8):e2330348. doi:10.1001/jamanetworkopen.2023.30348 ↩︎
-
Males on feminizing hormones face over double the risk of kidney stones.
A 2025 analysis1 of NIH medical records found that 10.3% of males on feminizing hormone therapy developed kidney stones, compared to 4.8% of those not on hormones. The risk was especially elevated for those on both estrogen and antiandrogens, with odds more than 2.5 times higher.
- Frangopoulos, E., Savin, Z., Gupta, K., Durbhakula, V., Gallante, B., Atallah, W. M., & Gupta, M. (2025). Increased Risk of Kidney Stones in Transgender Women and Gender-Diverse Adults on Gender-Affirming Hormone Therapy: Insights from a Large Database Study. Journal of Endourology. ↩︎
-
One in five vaginoplasty patients develop genital prolapse.
A 2025 Swiss follow‑up study1 (mean 27.5 years post‑surgery) found prolapse rates highest among those with peritoneal vaginoplasty (83%), followed by penile‑inversion techniques (17%) and intestinal vaginoplasty (14%). Surgical repairs often reduced symptoms but highlight long‑term complications rarely discussed before transition.
- Osswald, R., Villiger, A. S., Ruggeri, G., Hoehn, D., Mueller, M., & Kuhn, A. (2025). Twenty-Seven Years After Sex Reassignment Surgery in Female Transgender Patients: Is Prolapse of the Neovagina an Issue?. International Urogynecology Journal, 1-7. [Link] ↩︎
-
More than a third of UK residents in a survey did not know that “transgender women” are male.
More than a third of UK residents in a 2023 survey1 by Murray Blackburn Mackenzie—a Scottish independent policy analysis collective—did not know that “transgender women” are natal males. The findings show significant misunderstanding of the term and emphasize the need for clearer language in policy and media communication.
- Murray Blackburn Mackenzie. (2023, August 7). Clarity matters: How placating lobbyists obscures public understanding of sex and gender. Murray Blackburn Mackenzie. [Link] ↩︎
-
Around 25–50% of transmen and 5–10% of transwomen have had genital surgery.
Based on a 2019 review, genital surgery1 as part of medical transition is generally less common than chest surgery, with reported rates of 25–50% for transmen (natal females) and 5–10% for transwomen (natal males). These estimates come from a range of surveys and clinical reports.
- Nolan, I. T., Kuhner, C. J., & Dy, G. W. (2019). Demographic and temporal trends in transgender identities and gender confirming surgery. Translational andrology and urology, 8(3), 184. [Link] ↩︎
-
Estrogen use in trans-identified males is associated with a wide range of serious health risks—including blood clots, stroke, cancer, infertility, and cognitive decline.
A 2025 review1 summarizes wide-ranging risks tied to estrogen use in trans-identified males:
- 2.2× higher risk of blood clots (VTE)
- Up to 10× higher risk of stroke after 6 years on estrogen
- 1.8× higher all-cause mortality compared to other males
- 22.5–40.7× higher risk of breast cancer vs. male baseline
- 3× higher risk of cardiovascular death with estradiol use
- 72% increase in insulin resistance after 1 year; additional 9% in year 2
- Reduced brain volume and slower processing speed with long-term use
- Cognitive decline and elevated depression markers over time
- Only 0–24% retain sperm production after starting estrogen
- 6.6× higher incidence of multiple sclerosis
- Case reports of pancreatitis, autoimmune flare-ups, and brain tumors (meningioma)
The review emphasizes that many of these risks are under-recognized in clinical practice, raising urgent concerns about safety and informed consent.
- Schwartz, L., Lal, M., Cohn, J., Mendoza, C. D., & MacMillan, L. (2025). Emerging and accumulating safety signals for the use of estrogen among transgender women. Discover Mental Health, 5(1), 1-17. [Link] ↩︎
-
Trans-identified females report higher rates of sexual assault than their male counterparts.
A study by Abern et al.1 surveyed 996 trans-identified adults and found that 50% of females reported experiencing sexual assault, compared to 37% of males.
- Abern, L., Diego, D., Krempasky, C., Cook, J., & Maguire, K. (2023). Prevalence of sexual assault in a cohort of transgender and gender diverse individuals. Journal of general internal medicine, 38(5), 1331-1333. [Link] ↩︎
-
In one survey of WPATH-affiliated surgeons, over half reported performing vaginoplasty on minors
A 2017 study by Milrod and Karasic1 surveyed 20 WPATH-affiliated surgeons in the United States about their experiences and attitudes toward vaginoplasty in minors. Of these surgeons, 11 (55%) reported having performed the procedure on minors, with patient ages ranging from 15 to “a day before 18”.
- Milrod, C., & Karasic, D. H. (2017). Age is just a number: WPATH-affiliated surgeons’ experiences and attitudes toward vaginoplasty in transgender females under 18 years of age in the United States. The Journal of Sexual Medicine, 14(4), 624-634. [Link] ↩︎
-
Intestinal vaginoplasty in patients with stunted penile growth from puberty blockers can lead to bowel inflammation, excessive discharge, persistent foul odors, and fecal leakage
A 2017 survey by Milrod and Karasic1 found WPATH-affiliated surgeons in the United States considered sigmoid- or ileum-derived vaginoplasty (using sections of large or small intestine) an option for patients who had used puberty blockers. These patients, who had sometimes used blockers for up to 3 years, had severely underdeveloped genitals, described as “11-year-old genitalia” or a “micropenis,” which complicated standard surgical techniques. However, this intestinal approach was associated with serious complications, including diversion colitis (inflammation of the repurposed bowel tissue), excessive secretion, persistent foul odors, and potential leakage of stool into the peritoneum (the membrane lining the abdominal cavity).
- Milrod, C., & Karasic, D. H. (2017). Age is just a number: WPATH-affiliated surgeons’ experiences and attitudes toward vaginoplasty in transgender females under 18 years of age in the United States. The Journal of Sexual Medicine, 14(4), 624-634. [Link] ↩︎
-
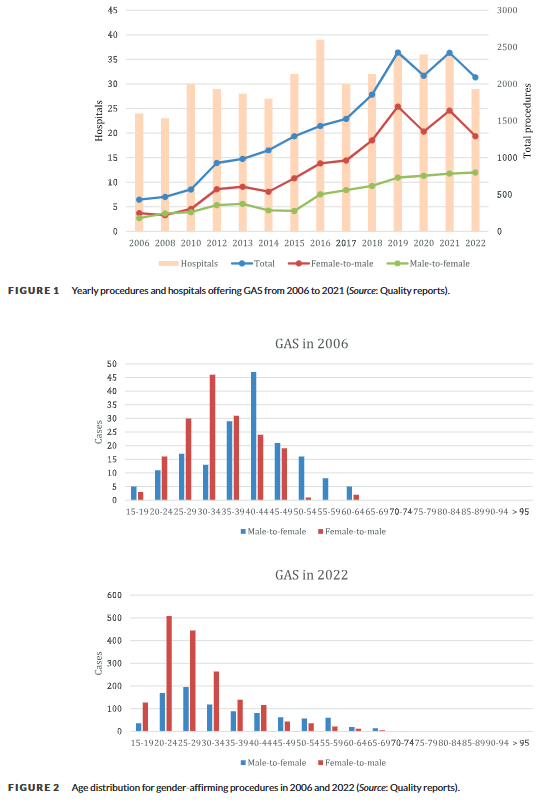
Genital masculinizing surgeries rose by 424% and feminizing surgeries by 343% in Germany between 2006 and 2022
A 2024 German national study1 analyzing hospital records found that genital “gender-affirming” surgeries increased nearly 5-fold between 2006 and 2022. Masculinizing surgeries showed the most dramatic increase at 424%, with their highest annual rise occurring between 2018-2019, while feminizing surgeries increased by 343%, with their steepest rise between 2015-2016. The study found a dramatic shift toward younger patients, with over 70% of masculinizing and about half of feminizing surgeries performed on people aged 20-34 in 2022, compared to about a quarter for both types in 2006. These procedures became increasingly concentrated in specialized centers, with half of hospitals performing over 50 masculinizing surgeries annually by 2022, up from 15% in 2006.
- Aksoy, C., Wellenbrock, S., Reimold, P., Karschuck, P., Ozturk, M., Hirsch, T., … & Flegar, L. (2024). Genital gender‐affirming surgery trends in Germany: Total population data with 19,600 cases from 2006 to 2022. Andrology. [Link] ↩︎
-
Suppressing sex hormones in males, using treatments like those prescribed as puberty blockers, is linked to an increased risk of dementia
A 2025 systematic review and meta-analysis1 found that men receiving androgen deprivation therapy (ADT) for prostate cancer had an increased risk of dementia, with a 26% higher likelihood for all types of dementia and a 9% higher risk specifically for Alzheimer’s disease, compared to men not receiving this treatment. ADT reduces the effects of male sex hormones (androgens) such as testosterone and dihydrotestosterone (DHT). This is achieved using medications, including GnRH agonists (which initially stimulate and then suppress hormone production via the pituitary gland), GnRH antagonists (which directly block hormone receptor activity), or through other pharmaceutical and surgical approaches. Notably, some of the same medications used for ADT—GnRH agonists, GnRH antagonists, and certain antiandrogens—are also employed as “puberty blockers” to delay puberty in children and adolescents.
- Ma, L., Tan, E. C., Goudey, B., Jin, L., & Pan, Y. (2025). Unraveling the bidirectional link between cancer and dementia and the impact of cancer therapies on dementia risk: A systematic review and meta‐analysis. Alzheimer’s & Dementia, e14540. [Link] ↩︎